To know Thalassemia
NEWS1. What is Thalassemia?
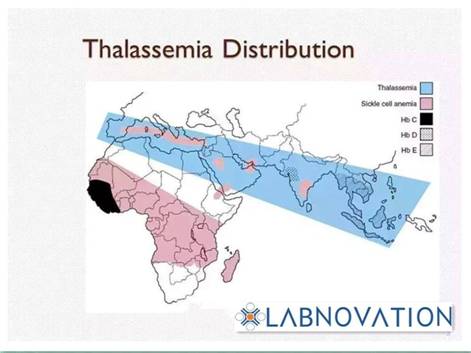
Thalassemia is one of the world's largest single genetic disease, especially common in the Mediterranean coastal countries, Southeast Asia and southern China. In high-risk areas of southern China, the crowded carrying rate ranges from 1-23%, Guangxi’s morbidity can reach 20%.
Thalassemia population distribution
Thalassemia is a latent inherited disease, if parents are gene-carriers of Thalassemia, their children have a quarter prevalence rate and a half rate of gene-carrier.
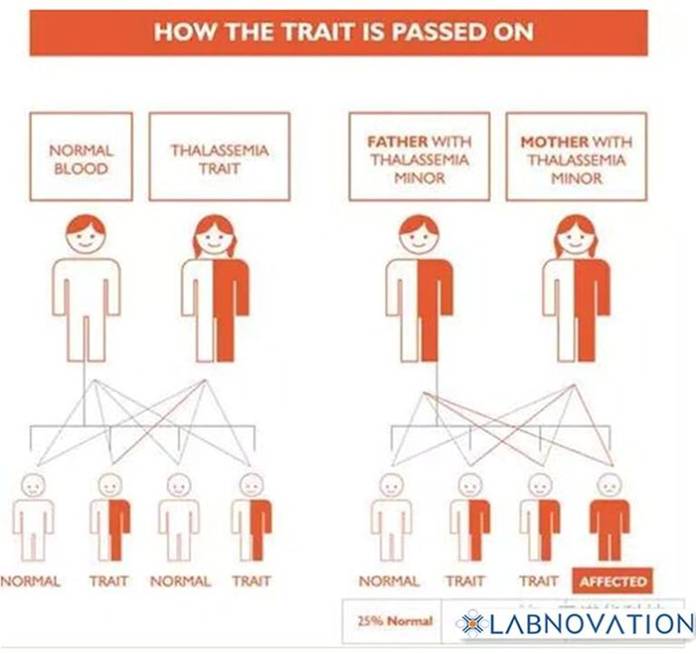
How the trait is passed on
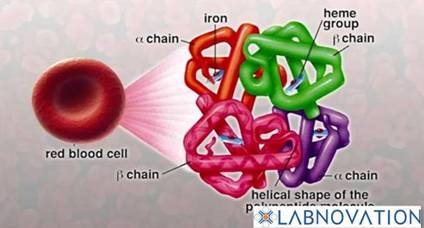
As genetic defects lead to different peptides synthesis(αβγδ) disorder, Thalassemia is usually devided into four types: α、β、δβ and δ,among them β and α are the most common. Clinically, the Thalassemia is divided into three grades: light, medium and heavy.
Hemoglobin Structure :
 α-thalassemia is mostly caused by gene loss. According to the amount of lack of gene,α-thalassemia is divided into four types:
α-thalassemia is mostly caused by gene loss. According to the amount of lack of gene,α-thalassemia is divided into four types:
Normal: Four genes in total(αα/αα).
α-thalassemia 2:1 gene deletion(-α/αα).
α-thalassemia 1: 2 genes deletion (--/αα)
HbH disease: 3 genes deletion(--/αα).
HbBart's Fetal edema syndrome :All 4 genes deletion(--/--).
β-thalassemia is mostly due to β memory point mutation。Some point mutations make beta chain completely unable to generate, which is called β0 thalassemia; some mutations only cause the beta chain to be lessen and called β+ thalassemia.
2. Clinical manifestations and laboratory tests of Thalassemia
Usually poor performance of the MCV decline, RBC brittleness decreased, β-thalassemia HbF increased and so on.
The difference between normal and thalassemia red blood cells:

Red Blood Cells
Laboratory tests include blood test (high sensitivity, low specificity),Erythrocyte brittleness (subjective), hemoglobin electrophoresis (specific for β-thalassemia than α thalassemia).
Diagnosis needs genetic testing, the most commonly used in clinic is α thalassemia(Gap PCR) and β thalassemia (PCR-RDB).
Anemia screening of thalassemia:
1)MCV <80fl or MCH <27pg, it is highly suspected to be thalassemia.
2)Erythrocyte osmotic fragility test positive (ROFT <0.6): can be suspected for thalassemia.
3)HbA2 <2.5%, is highly suspected to be α thalassemia gene carriers; ξ positive for the standard α thalassemia.
4)HbA2> 3.5%, then β-thalassemia gene carriers.
3.Thalassemia treatment
The current treatment of thalassemia is mainly regular blood transfusion, regular iron removal, (serum ferritin greater than 800-1000μg / L), the cost is high, bone marrow transplantation, around 4.5-6 million dollar.

Thalassemia
